You can access the full text of the MACRA draft rule at the Federal Register.
The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) represents a tectonic shift in how providers are reimbursed for the services they provide to Medicare fee-for-service (FFS) beneficiaries. MACRA shifts away from the financial certainty of fee-for-service reimbursement, adjusting provider reimbursement based on performance on quality measures, IT utilization, performance of clinical improvement activities, use of resources relative to peers, and participation in “Alternative Payment Models” (APMs). This is a major piece of legislation that will reshape the way in which healthcare is paid for. Furthermore, with MACRA implementation starting on January 1, 2017, providers need to understand how this soon-to-be implemented law will impact their reimbursement.
Q: How does MACRA affect reimbursement?
MACRA will have a major impact on the way most providers will be reimbursed for the care provided under Medicare Part B.
- MACRA permanently repeals the Sustainable Growth Rate (SGR).
- Under MACRA, Part B reimbursement will be adjusted. An eligible clinician1 will see his or her Medicare reimbursement adjusted under one of the three following options.
Figure 1: Options for Medicare FFS reimbursement adjustment under MACRAMIPS Partial qualified provider Qualified provider - Merit-based Incentive Payment System (MIPS) Adjustment to fee schedule (either positive or negative)
- Reimbursement through Advanced APMs does not meet threshold
- May choose MIPS adjustment or no adjustment to reimbursement
- Reimbursement through Advanced APMs meets Partial QP threshold, but falls short of full QP status
- 5% lump sum bonus payment
- Reimbursement through Advanced APMs meets threshold
- There will be no physician fee schedule updates from 2020 to 2025.2 Prior to any reimbursement adjustment, this may strain the budget of providers. When fee schedule updates resume in 2026, they will be higher for Qualified Providers (QPs).
The MIPS adjustment will vary by year, starting at -4% to +4% in 2019, and increasing to -9% to +9% in 2022 onward (actual positive MIPS adjustment will vary to target budget neutrality). While the adjustment is designed to be cost-neutral (and some providers will benefit from the MIPS adjustment) certainly the prospect of a downward adjustment to fees makes the certainty of QP status and the associated bonus all the more attractive. Providers who are not yet in a position to take on the two-sided risk that is a precursor to QP status will want to achieve a positive outcome by focusing on increasing their MIPS adjustment.
Q: Should I try to become a Qualified Provider?
There are a number of significant factors that need to be carefully considered when choosing to pursue QP status (as opposed to being subject to the MIPS adjustment), including the total financial risk in an Advanced APM and potentially higher net reimbursement under MIPS.
We expect that many providers participating in an Advanced APM will want the QP status (and the accompanying 5% bonus). To be classified as a Qualified Provider, two conditions must be met:
1) The eligible clinician must be associated with an Advanced APM. For now, this is limited to a small list of Centers for Medicare and Medicaid Services (CMS) programs that involve two-sided financial risk (among other requirements). It is worth noting that the aggregate financial risk in these Advanced APM arrangements is greater than the risk associated with the MIPS adjustment.
2) The Advanced APM must have a certain percentage of reimbursement or patient counts be associated with the attributed members of the Advanced APM. For example, for a Medicare accountable care organization (ACO), the numerator of this ratio might be the Part B reimbursement for attributed members, while the denominator is the Part B reimbursement for all attribution-eligible members.
For 2019, the claim dollar threshold for QP status is 25%, while the patient count threshold is 20%. However, these thresholds increase precipitously in later years. Both because there are relatively few Advanced APMs and the additional criteria for QP status are challenging, we expect that there will be relatively few Qualified Providers, especially in the early years of MACRA implementation. Furthermore, because Advanced APMs will be trying to meet the twin objectives of achieving shared savings and maintaining QP status, we expect these entities will carefully prune their networks to include providers whose practice patterns promote both organizational goals. Therefore, we expect that providers will be invited to join an Advanced APM rather than being able to elect to be included. While there may be a rush toward Advanced APMs, given the limited amount of CMS-approved APMs, organizations will need to carefully evaluate if they can understand the two-sided risk. Indeed, the 5% bonus3 would not offset the potential losses in these arrangements.
Q: How does the MIPS adjustment work?
The MIPS adjustment will adjust an eligible clinician’s fee schedule by a percentage value. The MIPS adjustment will vary by year, starting at +/-4% in 2019, and increasing to +/-9% in 2022 onward. The MIPS adjustment is designed to be cost-neutral. Beyond the cost-neutral MIPS adjustment, CMS will include a $500M “exceptional performance adjustment”4 for providers in the top three-quarters of those that receive a positive MIPS adjustment. This adjustment could represent up to an additional 10% on top of the existing MIPS adjustment for top performers.
Figure 2: MIPS adjustment
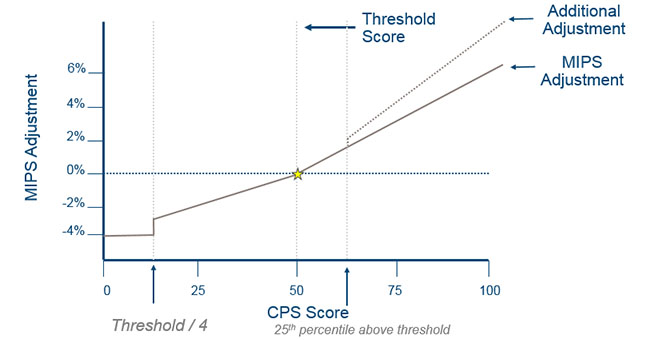
The MIPS adjustment is based on a provider’s Composite Performance Score (CPS), which is based on the average of four categories.
Q: How can I improve my chances of receiving a positive MIPS adjustment?
There are several actionable ways to improve the CPS, increasing the chances of a positive MIPS adjustment (and possibly an additional payment).
- In the Quality Performance category, you can report on more than the required measures and the top scores (subject to certain categorical constraints) will be included. Because quality measures are scored on a decile basis (think of it as scoring “on a curve”), your score is determined based on how you do relative to others who submit on the same measure rather than your absolute score.
- Also in the Quality Performance category, extra points may be obtained by submitting more than the required outcome measures, patient experience measures, completing the Consumer Assessment of Healthcare Providers Systems survey (CAHPS), and high-priority measures. Furthermore, additional points can be achieved by submission of quality measures through Certified Electronic Health Record Technology (CEHRT). The net impact of this extra credit can be up to 10%, which is substantial in the effort to break about the threshold score for MIPS reimbursement.
- The Resource Use category will measure the total resource use for patients attributed to the eligible clinicians relative to their peers. Although this category has a relatively small weight in the CPS for the 2019 adjustment (10%), this category will become more impactful in later years.
- The Clinical Practice Improvement Activities (CPIA) and Advancing Care Information categories are scored on an absolute basis. This means that you can earn a top score regardless of the performance of your peers. The CPIA requirements are relatively straightforward. Providers can use a smart strategy to obtain a high score for Advancing Care Information. Half of the 100 total points are achieved for reporting. The other 50 points are achieved through meeting certain goals. However, to reach the maximum score, 50 points must be achieved out of a total of 80 possible points. Because you don’t need perfect performance to achieve a perfect score, targeting certain Advancing Care Information categories where you are likely to see the most rapid improvement in the score will likely pay off.
- MIPS APMs have their composite performance score (CPS) weighted more heavily on the CPIA and Advancing Care Information categories, which are scored on an absolute basis. This may be an advantage for MIPS APMs.