The Centers for Medicare and Medicaid Services (CMS) introduced the Ambulatory Specialty Model (ASM), a new mandatory five-year risk model starting January 1, 2027, covering specialist care provided to beneficiaries with congestive heart failure or low back pain.
According to CMS, ASM is designed to “hold specialists who treat people with Original Medicare financially accountable for upstream management of chronic conditions.”1 CMS calls out that the two areas of focus, low back pain and congestive heart failure, have high Original Medicare spending, are managed primarily by specialists, and have significant potential for cost savings through avoidable hospitalizations and medically unnecessary surgeries.
ASM will build on much of the architecture in the Merit-based Incentive Payment System (MIPS) to measure clinician performance across four model performance measures, but ASM will focus most heavily on quality and cost performance. Using these four measures, clinicians will be evaluated by comparing their scores against other clinicians treating the same chronic condition. The result of this model will be an adjustment to each clinician’s total Part B payments in a future performance year of up to +/-9%, where the model is intended to be budget neutral for CMS.
ASM was introduced in the 2026 Physician Fee Schedule (PFS) proposed2 and final3 rules. Unless otherwise noted, all information contained here describing ASM is drawn from those rules, which were released on July 14, 2025 and November 5, 2025 respectively.
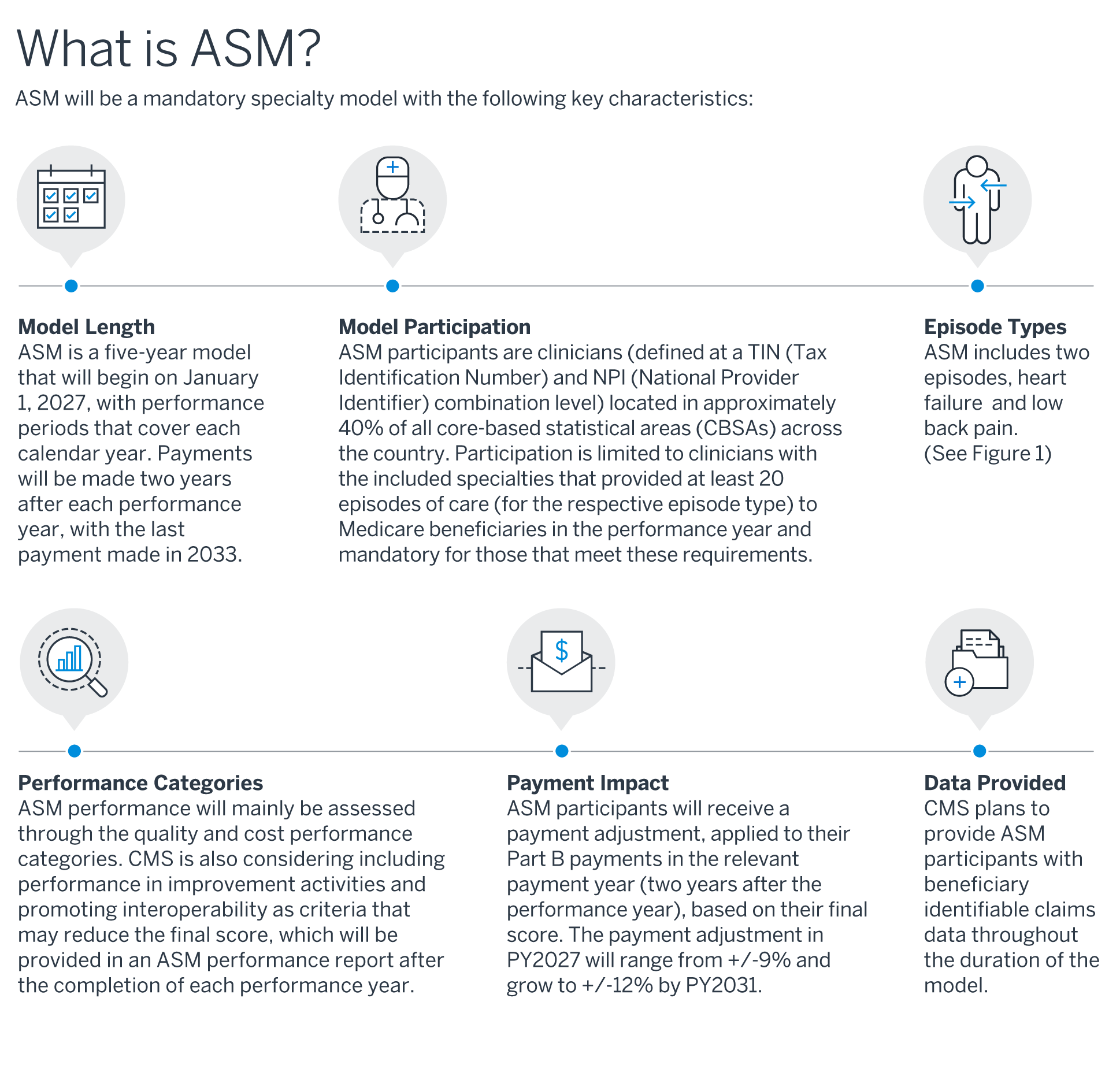
Figure 1: ASM episode types
| Heart failure4 | Low back pain5 | |
|---|---|---|
| Included specialists | Cardiology | Anesthesiology, pain management, interventional pain management, neurosurgery, orthopedic surgery, and physical medicine and rehabilitation |
| Episode length | 365–729 days depending on the continuation of care with the specialist | 120–484 days depending on the continuation of care with the specialist |
| Included services | − Cardiopulmonary procedures/interventions − Blood transfusions and associated labs − Services related to bleeding − Cardiac medications (injections, infusions, other forms) − Diagnostic imaging − Laboratory (panels, counts, smears, other analysis) − Outpatient visits − Other hospitalizations (complications and adverse drug events) − Aftercare, rehab, ancillary services − Durable medical equipment − Patient transport − Telehealth |
− Spinal surgeries and procedures − Hospitalizations − Spinal injections and neurostimulators − Imaging, diagnostics, and labs − Outpatient visits − Post-acute care services − Therapy services and manipulation − Telehealth − Medications − Behavioral health and ancillary services − Durable medical equipment − Patient transport |
Who is required to participate in ASM, and how will they be impacted?
Mandatory model and participation
CMS has tested a variety of episode-based models, the majority of which have been voluntary. Voluntary models are easier to implement and more flexible because they can be implemented without rulemaking; however, they are harder to evaluate and may generate less true savings due to selection bias and provider attrition. Mandatory models can help prevent (or at least minimize the impact of) these issues, while furthering CMS’s accountable care participation goals. Using the mandatory Comprehensive Care for Joint Replacement (CJR) model and Transforming Episode Accountability Model (TEAM) as foundations, CMS has been expanding their models’ geographic scope with a focus on CBSAs. This structure results in selection of a broader set of participants who are more representative of the U.S. population. CBSAs include both micropolitan and metropolitan statistical areas and reflect urban core populations of at least 10,000.
Similar to TEAM, to select eligible clinicians for participation in ASM, CBSAs and Metropolitan Divisions will be stratified into six cohorts based on the following criteria:
- Average total Parts A and B episode spending
- Volume of eligible episodes
- Metropolitan Division status
Within each of the six cohorts (summarized in the table below from 90 FR 32570), 40% of the CBSAs/Metropolitan Divisions will end up being selected for inclusion in the model.
| Cohort | Average total parts A&B episode spending* |
Volume of eligible episodes* |
CBSA or Metropolitan Division |
Number of CBSAs or Metropolitan Divisions in cohort |
|---|---|---|---|---|
| 1 | Low | Low | CBSA | 160 |
| 2 | Low | High | CBSA | 120 |
| 3 | High | Low | CBSA | 124 |
| 4 | High | High | CBSA | 136 |
| 5 | Very high | CBSA | 29 | |
| 6 | Metropolitan Division | 31 |
*Low = below median, High = above median, Very high = at or above the 95th percentile
If a CBSA/Metropolitan Division is selected, all eligible clinicians that meet the ASM eligibility requirements outlined below within those regions will be required to participate in the model. CMS plans to release information regarding the eligible ASM participants for performance year 2027 around Summer, 2026.
ASM participant eligibility
Clinicians within a selected CBSA/Metropolitan Division are only eligible for ASM if they meet all of the following participant eligibility criteria (90 FR 32565):
- Bills under the Medicare Physician Fee Schedule
- Bills the plurality of their Medicare Part B claims under one of the included specialty types
- Meets the episode volume threshold
- Using the MIPS episode-based cost measure (EBCM) a clinician must have at least 20 relevant attributed episodes to be included in the model.
ASM participant payment adjustment
All ASM participants for each cohort would be included in an “ASM incentive pool” that represents the total amount of funds used to determine the payment adjustment for each participant (90 FR 32605). The ASM incentive pool is calculated as follows:
(All Medicare Part B payments made to ASM participants during the performance year)
× (the ASM risk level)
× (redistribution percentage)
CMS specifies that the redistribution percentage would be set to 85% in 2027, and the remaining 15% will go to the Medicare Trust Fund. The risk levels for each performance/payment year are summarized in the table below (90 FR 32609).
| ASM performance year |
ASM payment year |
ASM risk level |
|---|---|---|
| 2027 | 2029 | 9% |
| 2028 | 2030 | 9% |
| 2029 | 2031 | 10% |
| 2030 | 2032 | 11% |
| 2031 | 2033 | 12% |
In order to distribute the incentive pool, CMS will transform the ASM participant’s score using a logistic exchange function. CMS does not specify the exact function they will use to transform the score, but it was chosen because it provides similar adjustments to participants with extremely high or low performance as are applied to participants with moderately high or low performance (i.e., it smooths out results at the extremes) (90 FR 32612).
The final payment adjustment percentage will then be used to adjust the APM participant’s total Part B payments in the payment year. For example, if an APM participant received an adjustment percentage of 3.5% for performance year 2027, they would receive an additional 3.5% of their 2029 Part B payments.
How is performance measured under ASM?
Each ASM participant will receive a “final score” in each performance year on a scale from 0–100 that will be used to determine their Medicare Part B payment adjustment in the payment year (90 FR 32598).
The final score for each participant is calculated based on the following four components:
- Quality: 50% weight
- Cost: 50% weight
- Improvement Activities: scoring adjustment of 0% to –20%
- Promoting Interoperability: scoring adjustment of 0% to –10%
Additionally, there are two score adjustments that are incorporated for (1) certain participants that serve a high proportion of complex patients and (2) for small practices (defined as a practice consisting of 15 or fewer clinicians).
- Complex patient: scoring adjustment of up to 10%
- Small practice: scoring adjustment of 10%
The stated reason for the downside-only weighting for Improvement Activities and Promoting Interoperability is that based on CMS’s research, many potential ASM participants would perform extremely well on both measures. By applying only downside impacts, CMS expects to see a greater distribution in ASM performance among participants and thus plans to reward high performance (90 FR 32599).
Quality measures
The quality component will be calculated based on a set of measures that will differ between heart failure and low back pain participants. The currently proposed measures for each participant type are summarized below (90 FR 32577):
| Heart failure | Low back pain |
|---|---|
| − Risk-standardized acute unplanned cardiovascular-related admission rates for patients with HF (MIPS Q492) − HF: Beta-Blocker Therapy for LVSD (MIPS Q008) − HF: ACE Inhibitor or ARB or ARNI Therapy for LVSD (MIPS Q005) − Controlling High Blood Pressure (MIPS Q236) − Functional Status Assessments for Heart Failure (MIPS Q3777) |
− MRI Lumbar Spine for LBP6 − Use of High-Risk Medications in Older Adults (Q238) − Preventive Care and Screening: Screening for Depression and Follow-Up Plan (MIPS Q134) − Preventive Care and Screening: BMI Screening and Follow-Up Plan (MIPS Q128) − Functional Status Change for Patients with Low Back Impairments (MIPS Q220) |
Each ASM participant would receive between 1 and 10 achievement points for each measure based on how the participant compares to measure-specific benchmarks. The benchmarks will be set based on the performance of other ASM participants in each measure, and points will be assigned based on the decile of performance to which the participant belongs for each measure. For example, if a participant is in the top decile for a certain measure, they will receive 10 of the 10 available points for that measure.
Cost measure
The cost component will be calculated based on the spending for each participant within the low back pain and heart failure EBCMs, respectively.
The cost measure score would be determined on a scale from 0 to 10, where a score of 6 is associated with the cost per episode for a participant being consistent with the median cost per episode of all ASM participants in that year. Costs above or below the median are assigned a score based on linear interpolation of the costs within each benchmark range (summarized below from 90 FR 32588).
| Benchmark range | Points | Calculation for the bottom of the range |
|---|---|---|
| Range 1 | 1–1.9 | Median + (2.5 x standard deviation) |
| Range 2 | 2–2.9 | Median + (2 x standard deviation) |
| Range 3 | 3–3.9 | Median + (1.5 x standard deviation) |
| Range 4 | 4–4.9 | Median + (1 x standard deviation) |
| Range 5 | 5–5.9 | Median + (0.5 x standard deviation) |
| Range 6 | 6–6.9 | Median |
| Range 7 | 7–7.9 | Median - (0.5 x standard deviation) |
| Range 8 | 8–8.9 | Median - (1 x standard deviation) |
| Range 9 | 9–9.9 | Median - (1.25 x standard deviation) |
| Range 10 | 10 | Median - (1.5 x standard deviation) |
Other considerations
As part of the Improvement Activities and Promoting Interoperability components, ASM participants must coordinate closely with primary care, including data sharing, supporting social needs screenings, and entering into collaborative care arrangements to strengthen communication and coordination. They must also utilize certified electronic health record technology (CEHRT).
To recognize the challenges faced by certain providers, participants treating more complex patients, such as those with higher medical and social risk, receive a score boost of up to 10%, as do small practices with 15 or fewer clinicians (including advanced practice providers) (90 FR 32603).
What support should potential participants consider for ASM?
ASM participants, both those familiar with and new to value-based care, should carefully consider their internal capabilities and seek outside support where they see resource limitations. Succeeding in ASM will not be solely about the participants’ quality of care—it will require managing relationships with other providers and understanding how their performance compares to other ASM participants.
ASM participants should consider reaching out to organizations that can provide the following support:
- CMS and MIPS bundled payment expertise: CMS continues to build upon its prior models, incorporating and improving past methodologies and measures. Organizations well-versed in these models can help participants navigate the process while providing insights for achieving success.
- Analytics: CMS models provide raw episode and claim-level data to participants on a regular cadence. Analytical support can help transform the detailed CMS data into reports or interactive tools that provide visibility into program performance in a user-friendly format.
- Benchmarks: As key components of the quality- and cost-scoring measures are derived by CMS based on ASM participants, it is beneficial to have access to utilization benchmarks to determine where your population ranks among your peers and to identify potential opportunities and risks.
Closing thoughts: how the Ambulatory Specialty Model will affect clinicians
Similar to the recent TEAM model, ASM will impact a wide array of clinicians in about 40% of CBSAs across the United States. These clinicians, both those familiar with and new to episode-based models, might not be able to fully realize opportunities and synergies that can be leveraged within the model.
Data alone will not change behavior or solve any inherent issues within a procedure or a clinician. Understanding the data, uncovering possible opportunities, and firmly committing to instituting changes are all necessary components of success. Milliman has extensive subject matter expertise and data-driven tools for episode-based programs to help highlight an organization’s areas for quality improvements and cost savings. For more information, contact your Milliman consultant.
1 Centers for Medicare and Medicaid Services. Model overview fact sheet: Ambulatory Specialty Model. Retrieved October 22, 2025, from https://www.cms.gov/files/document/asm-model-fact-sheet.pdf.
2 “Medicare and Medicaid programs; CY 2026 payment policies under the Physician Fee Schedule and other changes to Part B payment and coverage policies; Medicare Shared Savings Program requirements; and Medicare Prescription Drug Inflation Rebate Program.” (July 16, 2025). Federal Register. Retrieved October 22, 2025, from https://www.federalregister.gov/documents/2025/07/16/2025-13271/medicare-and-medicaid-programs-cy-2026-payment-policies-under-the-physician-fee-schedule-and-other.
3 “Medicare and Medicaid Programs; CY 2026 Payment Policies Under the Physician Fee Schedule and Other Changes to Part B Payment and Coverage Policies; Medicare Shared Savings Program Requirements; and Medicare Prescription Drug Inflation Rebate Program” (November 5, 2025). Federal Register. Retrieved November 14, 2025, from https://www.federalregister.gov/documents/2025/11/05/2025-19787/medicare-and-medicaid-programs-cy-2026-payment-policies-under-the-physician-fee-schedule-and-other.
4 Centers for Medicare and Medicaid Services. Quality Payment Program: Heart failure measure, Merit-based Incentive Payment System (MIPS), 2024 performance period. Retrieved October 22, 2025, from https://qpp.cms.gov/docs/cost_specifications/2023-12-05-mif-ebcm-heart-fail-v2.pdf.
5 Centers for Medicare and Medicaid Services. Quality Payment Program, Low back pain measure, Merit-based Incentive Payment System (MIPS), 2024 performance period. Retrieved October 22, 2025, from https://qpp.cms.gov/docs/cost_specifications/2023-12-05-mif-ebcm-low-back-v2.pdf.
6 Centers for Medicare and Medicaid Services. Specifications for Lumbar Spine Imaging for Low Back Pain Measure. Retrieved October 22, 2025, from https://www.cms.gov/files/document/lumbar-spine-imaging-low-back-pain-narrative-specifications.pdf.