Introduction: How the new CMMI LEAD model will serve populations dually eligible for Medicare and Medicaid
In December 2025, the Center for Medicare and Medicaid Innovation (CMMI) announced a 10-year Long-term Enhanced Accountable Care Organization (ACO) Design (LEAD) model. LEAD presents a new opportunity to serve populations with high health and social needs, including individuals dually eligible for Medicare and Medicaid. Although an early analysis from Milliman examines what is currently known about the model structure based on available guidance from CMMI, this paper takes a different lens.1 We focus specifically on LEAD's aim to support Medicare and Medicaid integration. In this article, we explore potential participation scenarios, highlight critical considerations for key stakeholders, and examine how different approaches could impact members, providers, ACOs, and states as the model details are released.
The LEAD model signals CMS's recognition that caring for complex populations requires more than traditional fee-for-service (FFS) incentives. Notably, CMS has emphasized its interest in innovative approaches to incentivize provider participation broadly, with particular focus on engaging providers in small practices and rural areas, settings that have historically faced barriers in health equity. CMS proposed the following model aspects that would support provider participation:
- Monthly upfront capitation payments
- Refined risk adjustment and benchmarking for individuals with complex care needs
- Incentives for primary care doctors to partner with specialists
- A 10-year performance period without rebasing benchmarks
- Additional payment targets for providers in rural areas.2
Characteristics of potential states participating in the Medicare–Medicaid LEAD model
CMS intends to select two states in the initial cohort to launch the Medicare–Medicaid LEAD model, one state with the majority of its Medicaid program in FFS and the other in managed care. Below are some additional characteristics of participating states that ACOs, providers, health plans, and states may want to consider before entering an ACO partnership for LEAD.
- Established ACO infrastructure. States with a significant ACO presence have provider organizations already familiar with shared savings arrangements, quality reporting, and care coordination requirements, which can accelerate implementation.
- Dual Eligible Special Needs Plan (D-SNP) market composition. States where a significant proportion of dually eligible individuals are enrolled in integrated D-SNPs (i.e., Highly Integrated Dual Eligible SNPs [HIDE-SNPs], Fully Integrated Dual Eligible SNPs [FIDE-SNPs]) may want to consider how a LEAD model would interact with existing programs and members’ continuity of care.
- Supportive legislative and regulatory environment. States with a history of legislative support for innovative delivery models may be better equipped to navigate the policy and operational requirements.
- Rural population concentration. With LEAD expected to include positive benchmark adjustments for rural areas, states with significant rural populations may find the model particularly attractive and better positioned to address long-standing challenges in rural provider participation.
Participation scenarios for providers and states in the Medicare–Medicaid LEAD model
CMS appears to recognize that no single approach will work across all markets and that innovation in model design may be necessary to address specific population and geographic needs. CMS intends to select two states for the first phase of the LEAD model and then work with those states during a planning phase to define the program’s financial and operational mechanics. Based on CMS's available guidance, many strategic considerations emerge for involved stakeholders.
ACOs and provider groups
For existing and future ACOs, the LEAD model offers an opportunity to receive federal support through a model designed to support enhanced quality of care and care coordination for dually eligible individuals. LEAD is unique in its design that ACOs partner with either an existing Medicaid managed care organization (MCO) or a state Medicaid program. LEAD ACOs that partner with an MCO or state Medicaid program will have the opportunity to align additional beneficiaries who are only enrolled in Medicaid with these organizations.
Provider organizations that already manage both Medicare risk through ACO participation or Medicare Advantage value-based arrangements and Medicaid risk through arrangements with Medicaid MCOs may be particularly well-positioned to launch a successful LEAD program, as they are already working to manage both funding streams for their dually eligible population.
Strategic considerations for ACOs:
- What additional care management tools or approaches could ACOs employ to better manage care for dually eligible beneficiaries?
- Which specialists do ACOs need to establish relationships with to help manage care for dual eligible beneficiaries?
- How does access to Medicaid services such as home and community-based services, non-emergency medication transportation (NEMT), and specialized behavioral health services impact health outcomes for dual eligible beneficiaries?
- How can ACOs work with community-based organizations such as Area Agencies on Aging (AAAs) to improve outcomes for dual eligible beneficiaries?
- How will the financial methodology account for the additional Medicaid services that would be covered by an individual ACO?
States
For states, LEAD may represent an opportunity to address a longstanding structural problem in financing care for dually eligible individuals. Under the current bifurcated system, states face misaligned financial incentives: investments in Medicaid-funded long-term services and supports (LTSS) can reduce Medicare spending by preventing hospitalizations and managing chronic conditions more effectively, but those investments increase state Medicaid expenditures while the Medicare savings accrue to the federal government. Several payment models—including the Financial Alignment Initiative (FAI) demonstration—have attempted to address this misalignment by creating mechanisms for sharing savings between federal and state governments.
The FAI demonstration ended in 2025 and states that participated in FAI, as well as states that have been seeking similar opportunities, may find LEAD appealing as a pathway to take on risk for Medicare FFS spending for their residents who are dually eligible for Medicare and Medicaid.
Given CMS’s stated intent to work with states that differ in Medicaid delivery approach and the flexibility in the model, the model could be appealing for many states, including the following:
- Washington’s FFS FAI demonstration model and investments in LTSS could make it an ideal candidate for the LEAD model if there is an opportunity for the state to share in Medicare savings.
- Vermont, with its significant emphasis on FFS delivery and ACO models for both Medicaid and Medicare, may also be interested in the benefits of a shared savings model.
- States such as Pennsylvania, with the majority of dual eligible individuals enrolled in a Medicaid managed care program (not including a D-SNP) or enrolled in a managed long-term service and supports (MLTSS) program, may benefit if they have a significant number of dually eligible individuals currently enrolled in traditional FFS Medicare.
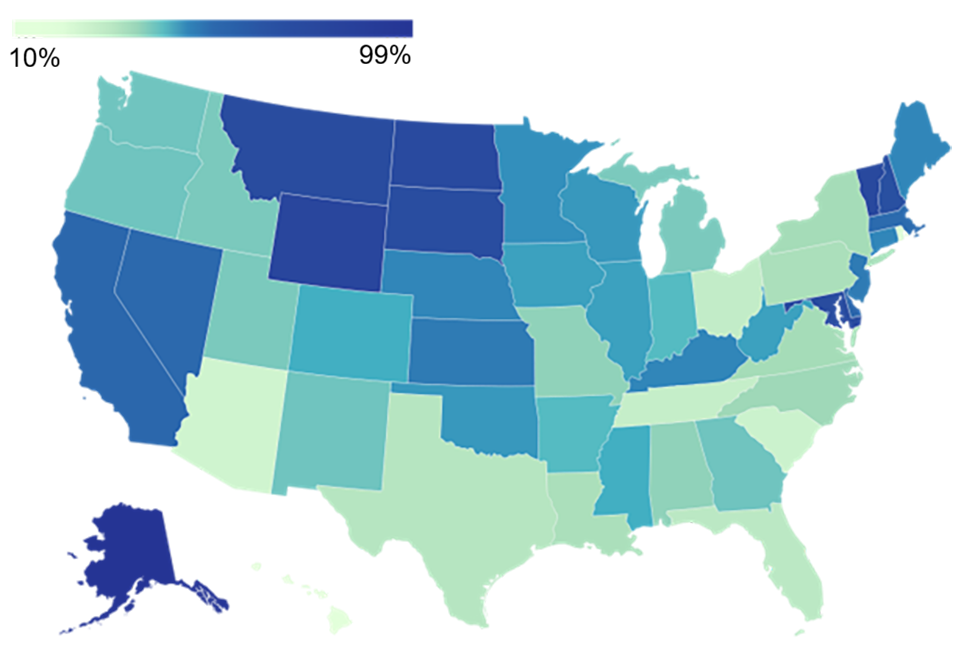
- Other states with a high proportion or large number of dual eligible individuals enrolled in Medicare FFS, especially in rural areas, may be interested in the model as a way to better coordinate care for dual eligible individuals. Figure 1 shows the proportion of full dual eligible individuals enrolled in Medicare FFS by state as of calendar year (CY) 2023.
- More than two-thirds of dual eligible individuals were enrolled in Medicare FFS in eight states: Alaska, Maryland, Montana, New Hampshire, North Dakota, South Dakota, Vermont, and Wyoming. Most of these states have a high proportion of the population residing in rural areas.3
- California has the largest number of dual eligible individuals enrolled in Medicare FFS.
Figure 1: Percent of dually elegible individuals enrolled in Medicare FFS by state
Strategic considerations for states:
States considering participation in the Medicare–Medicaid LEAD model should evaluate several key questions:
- What types of Medicaid managed care programs would be eligible for participation? For example, would state participation for the managed care option be limited to programs where all or nearly all Medicaid services are included in managed care, or would programs that carve out LTSS, behavioral health, or other services be excluded?
- What eligibility and enrollment mechanisms would limit disruptions in care for those individuals enrolled in the state’s integrated dual eligible programs? For example, is there a subset of the dually eligible population that may not be eligible for the states' integrated programs (e.g., under age 65)?
- How would the LEAD model interact with the state’s integrated dual eligible programs?
- What additional care management tools or approaches could states employ to better manage care for dual eligible beneficiaries?
- What additional Medicaid or waiver services would be beneficial for improving care coordination and driving long-term financial savings?
- How would the state savings portion be calculated? Would a state be required to pay a remittance to the federal government if a model failed to produce savings?
- Would states have authority to approve ACOs or define state-specific participation requirements?
Medicaid MCOs
Medicaid MCOs represent a third potential participant in the Medicare–Medicaid LEAD model, though their participation may be more nuanced. In the participating state with a managed care program for dual eligible beneficiaries, ACOs would have the option to enter partnerships with Medicaid MCOs. In this scenario, Medicaid MCOs could share in Medicare FFS savings for dually eligible individuals enrolled in the MCO's Medicaid program (often an MLTSS plan) but remain in traditional Medicare rather than enrolling in the MCO's D-SNP, if one exists. The framework for the partnership and savings calculation would be developed in collaboration with CMS through the planning phase and partnership agreements. Although this is an opportunity for Medicaid MCOs to participate in a Medicare ACO, the concept is not entirely new. CMS previously proposed a similar model through Direct Contracting Duals, which was not implemented but signaled federal interest in MCO accountability for Medicare FFS.4
Local and provider-sponsored health plans may be particularly well-positioned for this model. These plans often provide valuable perspective on complex members' needs, and provider-sponsored plans' affiliation with provider networks may enable more effective provider-plan collaboration to manage care. This could be especially appealing to CMS or states interested in engaging smaller plans with networks that include more independent and rural providers, the populations that LEAD specifically aims to serve.
Strategic considerations for MCOs:
- What types of Medicaid managed care programs would be eligible for participation? For example, would participation be limited to MCOs in comprehensive managed care programs (i.e., those providing Medicaid physical health, LTSS, and behavioral health services) or could MCOs in more limited programs (e.g., managed behavioral health programs) participate?
- What care management tools or approaches could Medicaid MCOs adopt to include Medicare-covered services?
- To what extent would MCOs be able to enter value-based arrangements with Medicare providers?
- For MCOs that also serve dual eligible individuals through an integrated program (e.g., FIDE-SNP), how do beneficiaries who opt for Medicare FFS in lieu of the integrated program differ from those who opt into the integrated program?
- Would enrollment in HIDE- or FIDE-SNPs be impacted by the existence of a Medicare–Medicaid LEAD ACO?
- How would state actuaries adjust Medicaid capitation rates to account for any impact on Medicaid costs?
How the LEAD model is poised to improve care for dually eligible individuals
The ACO LEAD model presents an opportunity to improve access and quality of care for populations with complex health and social needs while reducing overall health expenditures. For states, ACOs, health plans, and provider organizations willing to innovate, LEAD offers a pathway to address longstanding challenges in care coordination and financing for dually eligible individuals.
However, opportunity and complexity often arrive together. The level of technical assistance CMS will provide for LEAD remains unclear, and organizations considering participation should plan for the possibility that they will need to secure independent expertise to navigate model requirements, develop financial methodologies, and operationalize complex arrangements.
As this paper has illustrated, the LEAD model sits at the intersection of Medicare policy, Medicaid program design, provider risk arrangements, managed care operations, and actuarial methodologies. No single perspective is sufficient. Success requires teams that can translate between policy intent and operational reality, between federal requirements and state flexibilities, between financial risk and care delivery. This article brings together Milliman experts from across the healthcare policy and program spectrum to examine the Medicare–Medicaid LEAD model's implications from multiple perspectives: federal policy expertise, including at CMS's Medicare–Medicaid Coordination Office (MMCO); actuaries and consultants who support Medicare Advantage D-SNPs and state Medicaid agencies help develop programs for dually eligible individuals; and experts in provider risk-sharing models, including Medicare alternative payment models, such as Medicare Shared Savings Program (MSSP) and ACO Realizing Equity Access and Community Health (REACH). This cross-functional perspective allows us to consider how LEAD might unfold across different stakeholder groups.
As the healthcare market awaits additional details on the application process expected in March 2026, interested organizations can begin building readiness by:
- Assessing current capabilities against likely model requirements
- Identifying potential partners across the Medicare–Medicaid space
- Analyzing financial implications under different risk-bearing scenarios
- Engaging stakeholders early regarding governance and operational structures
For those seeking to deepen their understanding of the landscape LEAD will operate within, the authors recommend exploring additional resources on related topics:
- Key questions healthcare provider organizations should ask when evaluating LEAD
- 5 key issues Milliman is watching for ACOs in 2026
- Key insights into 2025 Medicare Advantage D-SNP landscape
- Medicaid long-term services and supports
- Direct Contracting Duals Model: Medicaid MCOs managing Medicare FFS costs for dual-eligible beneficiaries
CMS announced LEAD will have a 10-year performance period, and applications will be accepted in March 2026. Organizations that begin preparation now by building partnerships, assessing readiness, and securing the right expertise will be better positioned to seize the opportunity LEAD represents.
1 Kramer, E., Champagne, N., & Smith, C. (2026, January 8). Key question healthcare provider organizations should ask when evaluating LEAD. Milliman. Retrieved February 27, 2026, from https://www.milliman.com/en/insight/key-questions-healthcare-provider-evaluating-lead.
2 Center for Medicare and Medicaid Innovation. (2026, January 29). Long-term Enhanced Accountable Care Organization (ACO) Design (LEAD). Centers for Medicare and Medicaid Services. Retrieved February 27, 2026, from https://www.cms.gov/priorities/innovation/files/lead-model-overview-slides.pdf.
3 Centers for Medicare and Medicaid Services. (2025, September 30). CMS program statistics - Medicare-Medicaid Dual Enrollment. Retrieved February 27, 2026, from https://data.cms.gov/summary-statistics-on-beneficiary-enrollment/medicare-and-medicaid-reports/cms-program-statistics-medicare-medicaid-dual-enrollment.
4 Johnson, N, Shellabarger, S, & Hallum, A. (2021, February 3). Direct Contracting Duals model: Medicaid MCOs managing Medicare FFS costs for dual-eligible beneficiaries. Milliman. Retrieved February 27, 2026, from https://www.milliman.com/en/insight/direct-contracting-duals-model-medicaid-mcos-managing-medicare.